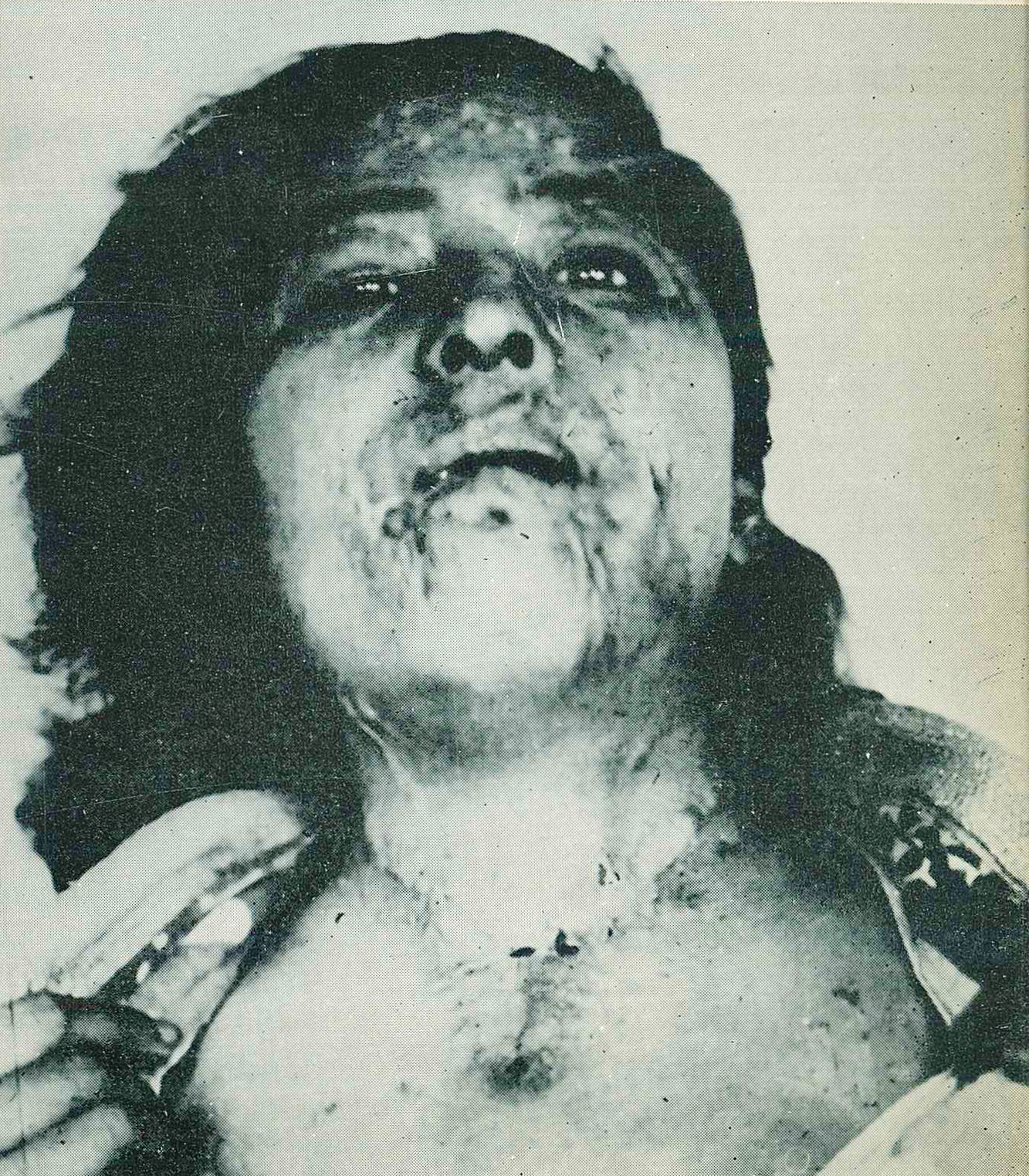
The detonation of the Hiroshima atomic bomb on August 6, 1945, caused ugly keloids on women who were exposed to the bomb, with skin stretched across their faces and chests. The keloid scars caused by the atomic bomb are physically and emotionally painful. Young women, in particular, felt emotionally guilty and vulnerable to the keloids on their faces and legs. Many scarred women fell into despair at the looks and words they received from those around them. The keloids left permanent scars on the victims' minds and bodies. Women with keloids, especially on their faces, often refused to leave the shelters or their homes, and women with keloids on their backs and shoulders were hesitant to show their skin. Many women wore long-sleeved shirts even in the summer after the atomic bomb attack.
While enduring emotional distress, many A-bombed women bravely sought ways to support themselves through collaboration with other peers who shared their condition. 1951 saw the formation of a self-help association for female keloid survivors by Reverend Kiyoshi Tanimoto. 1952 saw newspaper columnist Shizue Masugi and members of the Japan Penn Club In 1952, newspaper columnist Shizue Masugi and members of the Japan Penn Club notified some women of the plight of keloids and arranged for treatment in Tokyo to provide assistance to more women. Finally, the board of directors of the Hiroshima Peace Center in the U.S. sponsored some of the women to travel to the U.S. for treatment, and on May 5, 1955, 25 "Hiroshima Maindes" were selected by U.S. Air Force plane to travel to the U.S. for cosmetic surgery.
On May 5, 1955, 25 "Hiroshima Maindes" were selected on U.S. Air Force planes and headed for the United States for cosmetic surgery.
The name "keloid" refers to the irregular, abnormally protruding scar tissue that forms during the healing process of burned skin in atomic bomb survivors. The name comes from the fact that the scars look like crab shells and legs. The keloids, which are commonly seen at a distance of about 1.6 km to 2 km from the hypocenter, form about 4 months after exposure. They then become most pronounced at about 6 to 14 months. Most of the scars shrink and become scarred after about two years.
A relatively high incidence of severe scarring keloids and hypertrophic scarring occurs after the healing of second- or third-degree severe flash burns. Some people were assumed to have a predisposition to the development of scarring keloids. The late date of onset, the lack of complete and detailed ongoing research and documentation on a large number of cases dating back to the time of injury onset, and the multitude of variables made a complete assessment and analysis of scarring impossible. The high incidence of keloid formation, inadequate treatment, malnutrition, severe infections, and delayed healing affected the healing process, resulting in a high incidence of severe keloids or excessive scarring. Scarring keloids also occurred in burns from causes other than the atomic bomb. It seems most likely that scarring keloids do not represent a specific effect of the atomic bombs, as a similar incidence of scarring keloids could have occurred in burns of the same severity from other causes under similar conditions during the healing of lesions in patients with the same general state of health.
The etiology of keloids involves the detailed biophysical and biochemical processes that occur in the healing of skin lesions and the alteration of initial conditions and subsequent repair processes. In some cases, there is a tendency to develop excessive amounts of scar tissue in the healing of wounds. It is difficult to arrive at a sensible and practical definition of keloids. The most likely difference between a normal non elevated scar, a hypertrophic scar, and a cicatricial keloid is the difference in the amount of fibrous connective tissue that is produced during the healing process. Excessive collagen production, which causes scarring keloids and hypertrophic scars, occurs when it spreads deeper into the reticular layer. The dermis develops later as a result of necrosis caused by infection or additional trauma, with burns initially spreading to the depths of the dermis.