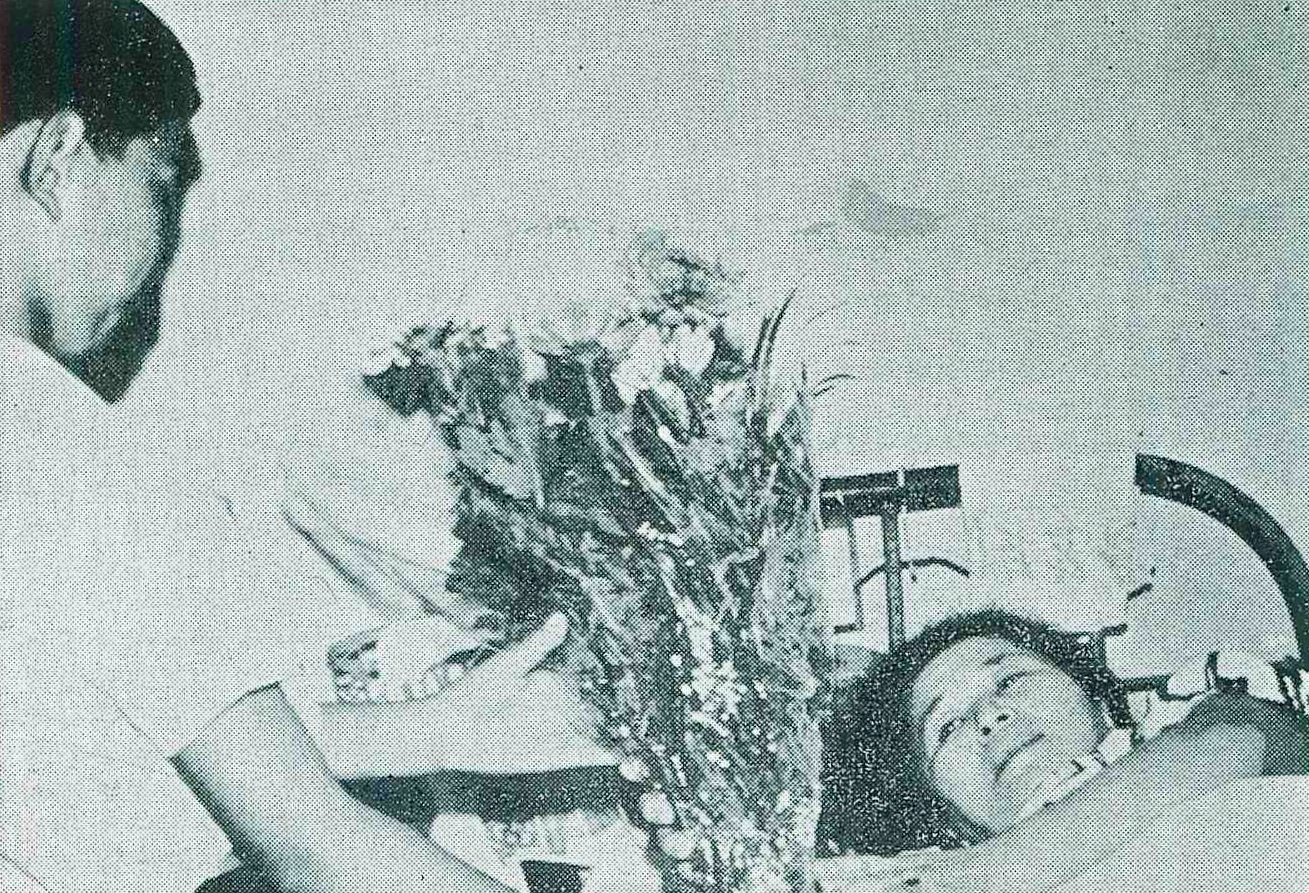
The children visited their mother with a bouquet of flowers after she was exposed to the Hiroshima atomic bomb and was admitted to the Hiroshima Red Cross Hospital for A-bomb Disease. Both the mother and the children were worried about the future development of A-bomb disease. The younger the child was exposed to the bomb, the higher the risk of contracting leukemia and other diseases. Hibakusha could not foresee their future lives and livelihoods.
The Hiroshima Atomic Bomb Survivors Hospital was operated to provide medical care for the survivors, and by 1969 had examined and treated some 44,293 people, with the number of patients peaking in 1955; in 1968 alone, some 442 people were hospitalized for leukemia and cancer, and some 63 people died of various cancers and leukemia.
The risk of radiation-induced leukemia differed from the risk of most solid cancers in two major ways. First, radiation caused a large percentage increase in the leukemia rate. Second, it tends to occur earlier after exposure to the atomic bomb, especially in children. The increase in leukemia began to appear about two years after radiation exposure, and the increase peaked about six to eight years after exposure. The risk of leukemia, like that of other solid cancers, depended to a large extent on younger age. Different types of leukemia are associated with different effects of age. Acute lymphoblastic leukemia was more prevalent among the young. Chronic myelogenous leukemia and acute myelogenous leukemia were more prevalent among sled elders.
The onset of leukemia was the most delayed sequelae of radiation exposure observed in atomic bomb survivors. Takuo Yamawaki, a physician in Hiroshima, was the first to discover an increase in the number of leukemia cases in clinical practice in the late 1940s. Subsequently, registries of leukemia and related disorders were established, and the first reports of increased leukemia risk were made in the early 1950s.
The incidence of leukemia caused by the atomic bombs was higher among those exposed closer to the hypocenter than from it. This increase first appeared about three years after exposure. From 1945, when the atomic bombs exploded, the incidence apparently reached its peak between 1950 and 1952. Since then, the incidence has declined, but for about 13 years after the bombing, it is still higher than what would be expected in the general population. The type of leukemia with the highest incidence was chronic granulocytic leukemia. Analysis of the data suggested a significant difference in the linear correlation between the incidence of leukemia and the incidence of leukemia when the radiation dose exceeded about 50 to 100 radians. Below this dose, the shape of the curve was not significantly different from the correlation.
The Radiation Effects Research Foundation (RERF) analyzed hundreds of thousands of residents of two cities, Hiroshima and Nagasaki, who were survivors after exposure to the atomic bombs. The RERF suggested that survivors were statistically significantly more likely to develop leukemia. In particular, those exposed at a young age, when their organs were still developing, had a particularly high incidence. Deaths from the development of stomach, liver, breast, ovary, and other major cancers were significantly higher among surviving survivors than among other subjects. The dropping of the atomic bomb that exploded in Japan not only killed hundreds of thousands of innocent civilians with its impact, but also caused many more deaths from atomic-bomb diseases and adverse health effects due to the persistent radiation from the radioactive nuclear weapons. After exposure to moderate and high doses of radiation, the likelihood of leukemia increased. After exposure to low doses of radiation, the incidence and risk of leukemia is unknown.